Anterior Cervical Discectomy with Fusion, One Level
 Anterior Cervical Discectomy with Fusion, One Level may be performed when a herniated disc pinches a nerve in the neck and non-surgical treatment has not resulted in sufficient relief. The primary symptoms of a Anterior Cervical Discectomy are usually numbness, weakness and/or pain in the arm and neck. The goal of the Anterior Cervical Discectomy with Fusion is to remove the disc that is pinching the nerve, eliminating the cause of pain and numbness. One level Anterior Cervical Discectomy with Fusion involves One Disc.
Anterior Cervical Discectomy with Fusion, One Level may be performed when a herniated disc pinches a nerve in the neck and non-surgical treatment has not resulted in sufficient relief. The primary symptoms of a Anterior Cervical Discectomy are usually numbness, weakness and/or pain in the arm and neck. The goal of the Anterior Cervical Discectomy with Fusion is to remove the disc that is pinching the nerve, eliminating the cause of pain and numbness. One level Anterior Cervical Discectomy with Fusion involves One Disc.
Preparation before surgery
You may be scheduled for presurgical tests (blood test, electrocardiogram, chest X-ray) several days before surgery. In the doctor’s office, you will sign consent and other forms so that the surgeon knows your medical history (allergies, medicines, vitamins, bleeding history, anesthesia reactions, and previous surgeries). Discuss all medications (prescription, over-the-counter, and herbal supplements) you are taking with your health care provider. Some medications need to be continued or stopped the day of surgery. Stop taking all non-steroidal anti-inflammatory medicines (Naprosyn, Advil, Motrin, Nuprin, Aleve, etc.) and blood thinners (Coumadin, Plavix, etc.) 1 to 2 weeks before surgery as directed by the doctor. Additionally, stop smoking, chewing tobacco, and drinking alcohol 1 week before and 2 weeks after surgery because these activities can cause bleeding problems. No food or drink is permitted past midnight the night before surgery.
Anterior Cervical Discectomy with Fusion, One Level Surgery
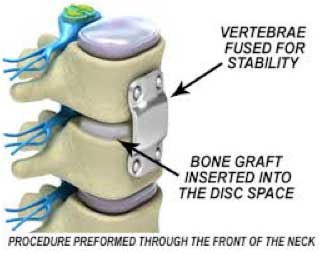
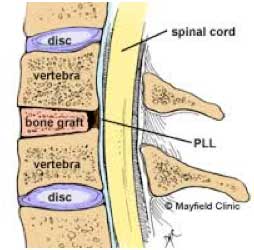 The incision is made in the front of the spine through the throat area. After the disc is removed, a bone graft is inserted to fuse together the bones above and below the disc space. Discectomy literally means “cutting out the disc.” A discectomy can be performed anywhere along the spine from the neck (cervical) to the low back (lumbar). The surgeon reaches the damaged disc from the front (anterior) of the spine through the throat area. By moving aside the neck muscles, trachea, and esophagus, the disc and bony vertebrae are exposed. Surgery from the front of the neck is more accessible than from the back (posterior) because the disc can be reached without disturbing the spinal cord, spinal nerves, and the strong neck muscles. Depending on your particular symptoms, one disc (single-level) or more (multi-level) may be removed. After the disc is removed, the space between the bony vertebrae is empty. To prevent the vertebrae from collapsing and rubbing together, a spacer bone graft is inserted to fill the open disc space. The graft serves as a bridge between the two vertebrae to create a spinal fusion. The bone graft and vertebrae are fixed in place with metal plates and screws.
The incision is made in the front of the spine through the throat area. After the disc is removed, a bone graft is inserted to fuse together the bones above and below the disc space. Discectomy literally means “cutting out the disc.” A discectomy can be performed anywhere along the spine from the neck (cervical) to the low back (lumbar). The surgeon reaches the damaged disc from the front (anterior) of the spine through the throat area. By moving aside the neck muscles, trachea, and esophagus, the disc and bony vertebrae are exposed. Surgery from the front of the neck is more accessible than from the back (posterior) because the disc can be reached without disturbing the spinal cord, spinal nerves, and the strong neck muscles. Depending on your particular symptoms, one disc (single-level) or more (multi-level) may be removed. After the disc is removed, the space between the bony vertebrae is empty. To prevent the vertebrae from collapsing and rubbing together, a spacer bone graft is inserted to fill the open disc space. The graft serves as a bridge between the two vertebrae to create a spinal fusion. The bone graft and vertebrae are fixed in place with metal plates and screws.
Recovery
Following surgery the body begins its natural healing process and new bone cells grow around the graft. After 3 to 6 months, the bone graft should join the two vertebrae and form one solid piece of bone. The instrumentation and fusion work together, similar to reinforced concrete. You must wear your collar at all times except to shower, and you may remove it briefly for personal hygiene (shaving). While the collar is off, you may look forward or slightly downward, but you must not look up. This motion extends your neck and can cause the bone graft to dislodge. Most people will need to wear the collar until the first post-operative appointment. At that time, I will determine if you are able to stop using the collar. In most cases, a collar will be worn for about 3-4 weeks. Some patients may have to continue to wear the collar for a longer period of time depending on their situation
Risks
Anterior Cervical Discectomy and Fusion (ACDF) is generally a safe and effective surgery. However, as with any surgical procedure, there are potential risks. Risks of the operation include, but are not limited to: infection, anesthesia complications, injury to the nerves and spinal cord, hoarseness, injury to the esophagus, incomplete resolution of pain, and dislodgement of the graft. General medical complications include pneumonia, heart attack, stroke and blood clots. These complications are uncommon, and many precautions are taken to prevent or minimize risks but because human biology is at times unpredictable, no surgery is risk free.