Medial Collateral Ligament (MCL) Reconstruction
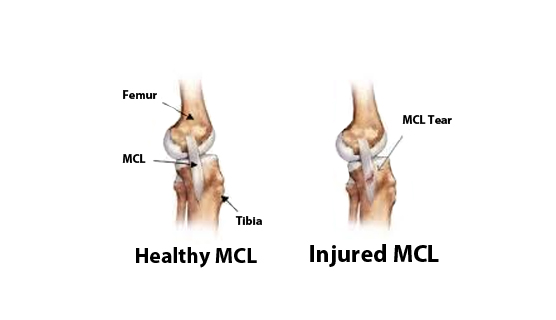
An injury to the Medial Collateral Ligament (MCL) occurs when there is a stretch, partial tear, or complete tear (rupture) to the ligament. The medial Collateral Ligament (MCL) is a wide, thick band of tissue running down the inner knee from the thighbone (femur) to a point on the shinbone (tibia) about four to six inches from the knee.
The Medial Collateral Ligaments main function is to prevent the leg from extending too far inward, but it also helps keep the knee stable and allows it to rotate.
Preparation for the Medial Collateral Ligament Reconstruction
Preparations depend on your surgeon. In general, you should:
- Avoid certain medications. Your doctor may want you to avoid taking medications or dietary supplements that can increase your risk of bleeding.
- Fast beforehand. Depending on the type of anesthesia you’ll have, your doctor may want you to avoid eating, or drinking six to twelve hours before your procedure.
- Arrange for a ride. You won’t be allowed to drive yourself home after the procedure, so make sure someone will be available to pick you up. If you live alone, ask someone to check on you that evening or, ideally, stay with you the rest of the day.
- Choose loose clothing. Wear loose, comfortable clothing baggy gym shorts, slip on shoes for example, if you’re having knee arthroscopy so you can dress easily after the procedure.
Medial Collateral Ligament (MCL) Surgery
When MCL surgery is done, it is usually done through a small incision on the inside of your knee. It is not done arthroscopically, since this ligament is not inside the knee joint.
If the medial collateral ligament has been torn where it attaches to the thighbone (femur) or shinbone (tibia), the surgeon will re-attach the ligament to the bone using large stitches or a metal screw or bone staple. If the tear was in the middle of the ligament, the surgeon will sew the torn ends together.
RECOVERY
On average, it takes six weeks for a Medial Collateral Ligament (MCL) Reconstruction to heal. The initial treatment for most MCL tears focuses on reducing the pain and inflammation in the knee while immobilizing the knee to keep it stabilized. This includes:
- Resting, icing and elevating the knee
- Taking pain relievers, such as aspirin and ibuprofen, to ease pain and swelling
- Wearing a lightweight cast or brace that allows your knee to move backward and forward while restricting side-to-side movement. It usually is recommended to keep the knee immobilized like this for 72 hours, depending on the severity of the injury. The cast or brace may be designed so that you cannot bend your knee at all. If this is the case, you will need to modify your behavior so that you can avoid having to squat, kneel down or bend over.
- You should try to keep your leg elevated even if you are sitting in a chair, to reduce blood flow to the knee.
- Once the pain and swelling subside, you will begin rehabilitation, which will include exercises to restore strength and normal range of motion to your knee.
- If your knee feels sore while you are doing these exercises, you should proceed slowly to prevent further irritation
Risk
Managing risk:
-
- The most effective treatment of complications is prevention. For example, the risk of infection is decreased by giving antibiotics prior to surgery
- The risk of blood clots is decreased by using anti-embolism stockings.
- Knee stiffness can often be managed with physical therapy and braces.
- Since most complications can be effectively managed when identified promptly, if patients have questions or concerns about the post-operative course, the surgeon should be informed as soon as possible.